Take The Prediabetes Risk Test | DoIHavePrediabetes.org has a visual step-by-step questionnaire to assess prediabetes risk without a blood test.
risk to kidney.. if and only if diebetes is poorly managed, then kidney can be damanged, according to Dr Cindy of RMG
— aging calls for diet adjustment .. As our organs (like pancreas) age, t2dm (Type2 Diabetes mellitus) risk increases, so it’s wise to adjust diet habits early in your life
* Tier 1 important factors for me .. cakes/sugary-desserts/chocolates; sweet fruits;
* Tier 2 factors for me .. (refined) starch; belly fat
** Obvious but Tier 2 factors for me .. sugary drinks; visible sugars
Avoid or reduce
- white rice , yellow noodle
- fruit juice .. esp. at airplanes or parties. These are seldom real juice.
- milk chocolates, chocolate-flavored <whatever> (always too sugary)
- grapes, sweet mangos, sweet oranges, durain,
- all fruit-flavored foods .. flavor invariably comes from added sugar, never real fruits
If I can’t reduce to “two fruits a day”, then I will go for less sweet fruits like pear, kiwi, variouis berries,
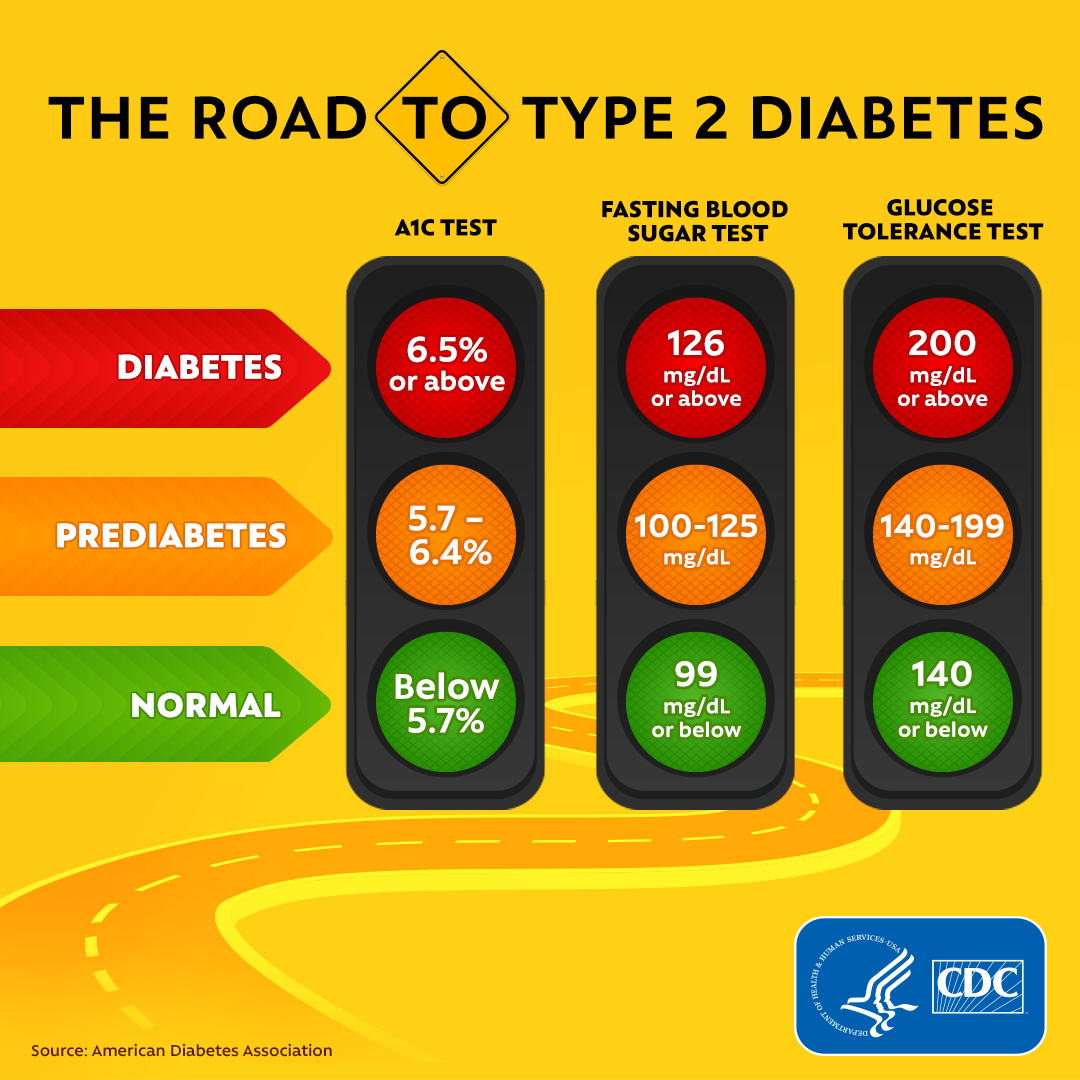
— compare the three diagnostics
CDC_Diabetes_Social_Ad_Concept_A2_Facebook.png (1080×1080) is a visual chart comparing all three
Some overseas publications (esp. from U.S.) say Hba1c is more accurate than FPG, though Singapore MOH approved FPG before hbA1c. For future blood tests, include both. OGTT (most time-consuming) is the gold standard diagnostic, and is used in uncertain cases.
Dr Cindy of RMG said that a clean OGTT means that 5.9% Hba1c is not a real concern. You can retest OGTT annually iFF Hba1c is 5.7% or higher.
I told Dr Lau that my hbA1c may remain in 5.6 ~.5.9. Still, she felt it doesn’t mean I’m prediabetic.
Dr Lau said OGTT level 120 is what she looks for, though 140 is official diagnosis for prediabetes.
( for FPG 100 mg/dL is the cutoff. Am 90.)
Hui Mei said usually the FPG will detect pre-diabetic earlier, even when hba1c is still normal. I think that is logical — Hba1c is slower to change and shows less fluctuation.
Q: some sites (CDC and Mayo clinic) classify Hba1c 5.7% as prediatetic, but presumably most patients will skip OGTT and live with the assumption for decades?
A: ….
— hb A1c history
- 5.6% 20 Feb 2025
- 5.5% 5 Nov 2024
- 5.4% 4 Apr 2024, big improvement.
- 5.9% 3 Jan 2024 ICON
— Prediabetes .. reversible, but t2dm is probably not. Reversal requires lifestyle improvements. I think that’s the rationale of the “prediabetes” designation, diagnosis, public education, public funding,,
Compared to other countries, U.S. researchers, healthcare providers, governments and publications emphasize pre-diabetes.
HuiMei said U.S. cutoff (5.7%) is for U.S. population, with its own ethnic makeup. Indeed hbA1c is race-specific. Still I find 5.7% an important reminder for me to improve diet habits and maintain the (shrinking) buffer zone from prediabetes.
— prevalancce of diabetes .. Age-adjusted prevalence calculation factors in the strong pattern that older people are more likely to develop t2dm. https://www.moh.gov.sg/news-highlights/details/result-from-government%27s-five-year-war-against-diabetes-effort shows 8% among Singaporeans.
Many people are predisposed due to genetics and adopted lifestyle of family and community. My CAD condition makes me more vulnerable to t2dm than most people. I may not be predisposed, but am still high-risk.
{kind=link}